PT Crab 🦀 Issue 141 - Let’s get nervous
This week, we’re talking about nerve injuries. Specifically, upper extremity nerve injuries. Even more specifically, actually that’s as specific as we get today. This week’s edition only has two pieces, the first a huge review of upper extremity peripheral nerve injuries in throwing athletes. It’s told from a medical perspective, so there’s not a lot of physical therapy treatment to go after, but it’s a fantastic diagnostic resource. The second is quite specific about the treatment of suprascapular nerve entrapment syndrome. And the third doesn’t exist, like I said, because I’m going deep on the first one.
Also this week, it may be the height of summer and it may be the hottest summer ever (so far), but it’s time to start thinking about leaves. If you want to get away to see some fall foliage like the bourgeoise person you are, you’re gonna need to get that planned. In Virginia, where I am, we’re looking at late October for the peak in the Blue Ridge, about two weeks before I’m running my first (and maybe only, we’ll see) ultramarathon. But more on that in the future. For now, here’s the map to plan your fall trip with week by week predictions of the best time to see foliage in your area.
With that, let’s dive in!
All the UE Nerves, Everywhere.
The Gist - This is going to be a long gist. You’ve been warned.
This article breaks down common injury mechanisms and diagnostic tests for upper extremity nerve injuries in throwing athletes and it really dives in. Fortunately, there are some really handy tables that you can refer to if this is a population that you regularly see. For evidence of importance of all this, a recent study showed 1.26 injuries per 1000 “athletic exposures” (e.g. games and practices) in high school baseball players. With 5 day a week practices/games for four months at this level, that’s a lot of injuries. The article has a nice breakdown of the biomechanics of overhead throwing at the beginning, so if you’re rusty on that you can give it a look as well.
For the nerves, I’ll do a quick breakdown of which they looked at and the common signs and symptoms of each.
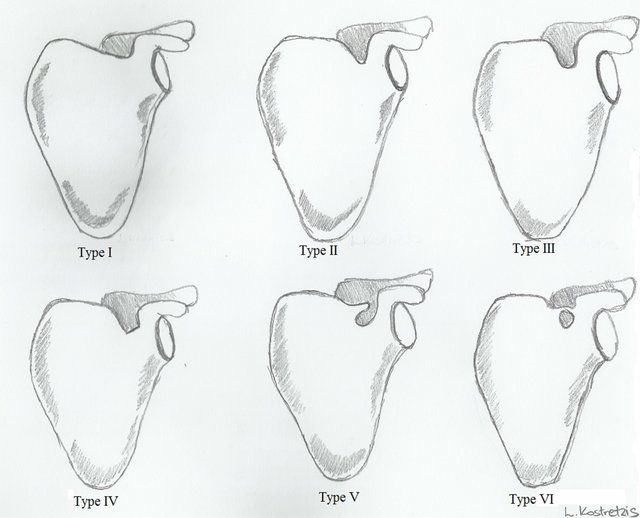
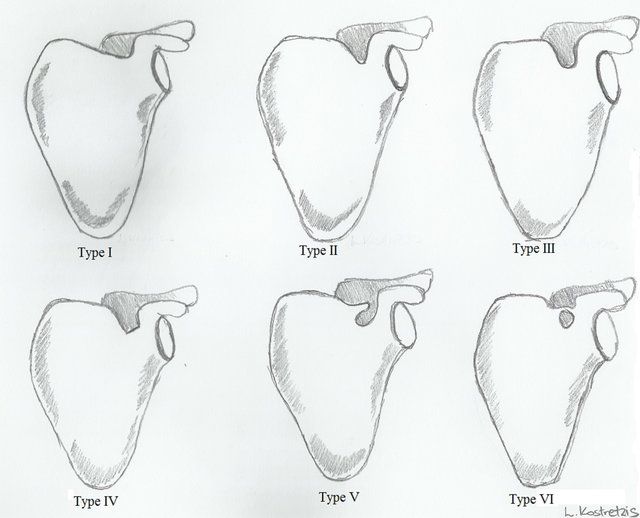
- Suprascapular nerve
– Vague, deep posterior shoulder pain – Shoulder abduction and ER weakness – Scapular dyskinesia – Infraspinatus atrophy - Axillary nerve
– Pain and decreased sensation in lateral shoulder – “Dead arm” feeling with overhead activity – Weakness of flexion, abduction, or ER - Ulnar nerve
– Decreased throwing velocity, accuracy, or endurance – Medial elbow pain – Loss of grip strength or clumsiness in hand - Radial nerve
– Lateral elbow and dorsal forearm pain worsened with resisted supination with 90 degree flexed elbow – Tenderness distal and anterior to lateral epicondyle – Weakness with finger extension - Thoracic outlet
– Vague pain, numbness, and parasthesia of throwing arm - Long thoracic nerve
– Vague shoulder pain and decreased endurance – Scapular winging - Musculocutaneous nerve
– Elbow/forearm pain – Weakness with elbow flexion –Numbness/parasthesia over dorsal forearm - Median nerve
– Vague proximal forearm or antecubital pain – Numbness in median distribution – Weakness with pronation, wrist flexion, or grip strength
Phew that was a lot. And those are just signs and symptoms from the table. Each nerve has about a paragraph that fleshes out the information above and more paragraphs on treatment. The paper also goes through the etiologies of these nerve injuries and diagnostic methods. Diagnostic methods in this paper are aimed at physicians, so you’ll see a lot of EMG/NCS and injections, but there are also physical diagnostic signs included.
If you work with upper extremity injuries at all, this paper is definitely worth a read to refresh yourself, I found it to be invaluable.
Tell Me More - How about treatment? As you may expect from a paper written by physicians, most treatment information is intended for physicians, so not super useful for physical therapy. There are some details about a PT approach, but most of them you’ll find quite obvious. Instead of going into that information, I’m going to tell you about some general considerations.
For one, the paper points out that “a Cochrane review noted very low-quality evidence with no indication of any significant neuropathic pain and symptom reduction with NSAIDs,” and that common neuropathic agents that are effective at low doses can cause lethargy and dizziness, so they should be used cautiously.
And now I’m going to sprinkle in some notes about different nerves that you may find clinically useful. For example:
- Ulnar nerve
– The traction and compressive forces at the elbow due to cocking and acceleration in throwing and the excessive valgus force combined with elbow extension all open up the nerve to injury. “Flexor carpi ulnaris contraction with the elbow flexed in the throwing motion can increase pressure in the cubital tunnel from 6 to 20 times,” and the ulnar nerve elongates 4.7mm with elbow flexion, so it’s quite exposed to hazards. - Long thoracic nerve
– “Etiology is generally an overuse traction injury with the head tilted or rotated away from the throwing arm as it is overhead.”– “Overuse long thoracic nerve injuries in throwing athletes typically spontaneously resolve with nonsurgical management in 6-18 months.” n.b. they say spontaneous, but I know physical therapists are actually fixing these folks. - MSC nerve
– “The nerve is commonly injured in the distal arm owing to overuse that includes forceful pronation of an extended elbow… more specifically, overstretching of the nerve may occur at ball release through deceleration.”
Since I’ve crossed 1,000 words, I’m going to leave this paper here for your reading pleasure. There’s a lot of great stuff in this dense paper, so I highly recommend you give it a read. The last note I have is that the authors say that many of these nerve injuries occur alongside injuries to other structures, so keep an eye out whenever you’re assessing the shoulder. K? Bye!
Paper? Gots ya.
Having trouble staying hydrated at work? Try something new.
The Gist - Hint is a fruit-infused water that’s been taking the world by storm recently. It has no calories, no sweeteners, no sugar, and no need to go to a store to buy. They’ll ship it right to you!
They have a $45 off deal for PT Crab subscribers going on right now, available through this link. Just $36 for three cases of fruit-infused water, and PT Crab makes money when you buy too, so it’s a win-win.
Seriously, this stuff is great, and it comes in coconut flavor which is objectively the best flavor. It just is.
So try Hint Water today!
And that’s our week! Thanks for supporting PT Crab an do consider trying out Hint Water. Since you’re getting the Crab for free, I keep it running via ads like this one, but I only get paid if you try the deals, so at least give it a look! And if you don’t like ads (who does?) then become a supporter, they get 3x the articles and no advertisements for just $5 per month.
Bye!



Comments
Want to leave a comment and discuss this with your fellow PTs? Join PT Crab and get summarized PT research in your inbox, every week.