🦀 PT Crab Redux - Issue 73 - The Walk and Talk
This week I’ve had to resort to rehashing an old edition of the Crab, from almost exactly a year ago. That’s because the internet hasn’t been working where I’m staying for about the last 5 days and this week’s issue can’t be published without it. :( So I’m using my phone to write this intro and will be back to you next week with a brand new edition. Sorry! In the meantime, the whole archive is available at PTCrab.org. Find anything you need by searching there. ’Til next time!
A walk and talk is a television classic, thanks Aaron Sorkin and The West Wing. I imagine most of you are too young for the show (and, unfortunately, it doesn’t really hold up) but trust me, it has influenced a lot about how we watch TV. Most of you are certainly too young for I Love Lucy as well (possibly all of you are) but I grew up watching it on TV Land and so I’m super excited for Aaron Sorkin’s new project, Being the Ricardos, coming out next week. Desi Arnez completely changed TV production with his filming techniques and his deal that gave him the rights to the negative of the show and Lucille Ball was the first pregnant woman to regularly appear on a TV show. CBS didn’t think anyone would want to watch reruns, Desi knew better and history was made.
But I very digress even more than usual. This has nothing to do with this week’s topics, outside of the walking part. This week, we are walkin’ as we assess the association between daily walking and the risk of knee replacement in people with OA and the treatment of cuboid syndrome (which I apparently have). Our King Crab supporters got an extra article this week, one that looks at long term outcomes of conservative management of idiopathic toe walking and it’s a doozy.
If you want more articles and/or want to support PT Crab, subscribe here.

With that, let’s dive in!
A Walk a Day Keeps the TKR Away
The Gist - If you’ve already got knee OA, walking helps push off TKR. That’s what this prospective observational study from the Archive of PM&R told us at least. They examined the association between the volume and intensity of daily walking and the risk of knee replacement over five years in people with advanced knee OA to discover that. Specifically, replacing 10 minutes per day of very light or light walking with moderate walking reduced the risk of knee replacement by about 36%. IDK about you, but I think that’s a lot. They followed these people for 48 months(!) and got accelerometer data from 2,127 of them that led them to their conclusions.
For those conclusions, level of walking (light, moderate, etc.) was determined by step rate, with >100 steps being classed as moderate and 50-100 as light. Interestingly, total walking volume didn’t change TKR risk, but walking intensity did. Most importantly, neither walking volume nor intensity increased the risk of TKR over the course of five years. That’s some good news.
Tell Me More - You may have already spotted a complication of the protective effect of daily, moderate walking (which this study demonstrates to be quite protective, that’s the 36% reduction part). People often walk more slowly when they have more functional problems or more pain regardless of apparent structural deformity (that’s how these people were classified). TKR is often associated with less function or more pain. So this study is saying that those who walked harder had fewer TKRs without checking for confounders like pain, outcome measures, etc. I’m not usually one to criticize studies since that’s not my expertise, but I thought it was worth pointing out. Again though, the main point of the study is that no volume or intensity of walking they saw made TKRs more likely and that’s great news.
I do recommend reading the whole study for more details since it’s not too complicated and potentially quite useful in patient education. Before going, I’ll just point you to my favorite part of the paper:
One potential strategy to increase daily walking is to consider referral to a physical therapist because physical therapists are experts in prescribing exercise for adults with chronic disease and can educate patients about the benefits of exercise while addressing knee pain and limitations in physical function. Physical therapy is likely underutilized for knee OA.
#agree
Paper? But of course.
Cuboid Syndrome Apparently Exists
The Whole - This literature review from the journal Sport Physical Therapy (and from 2011) is about Cuboid Syndrome, an interesting condition that I thought I’d highlight because I have it. If you want information about your own conditions, write your own newsletter! (But actually, if you want information about anything in particular, email me and I’ll get it in a future Crab. Or just start your own newsletter, it’s fun. Sometimes.) Cuboid syndrome, according to the paper, “is an easily misdiagnosed source of lateral midfoot pain, and is believed to arise from a subtle disruption of the arthrokinematics or structural congruity of the calcaneocuboid.” It most commonly occurs along with a lateral ankle sprain, but can develop chronically in athletes, usually dancers. Basically, this super stable joint gets unstabled by the fibularis longus tendon yanking it out of position. The tendon loops under the cuboid (see the photo, it cleans things up in your head)
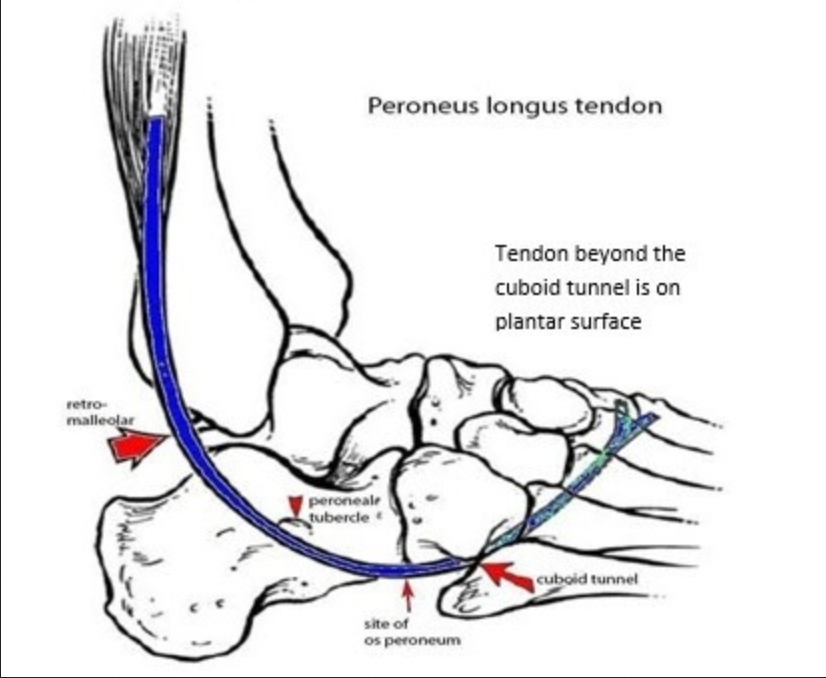
and chronic uncontrolled pronation can pop it out of place. Unfortunately and fortunately, this out-of-placeness is very minor, so much so that it can’t be seen on radiographs.
How do we know it’s messed up then? Tests my dear Watson. There are quite a few things that can cause lateral foot pain, as I’m sure you know so you have to screen those out as best you can. Fortunately, the best way to diagnose it is by treating it. If the manipulation for it works (the cuboid whip), then it’s probably cuboid syndrome. Padding under the cuboid to help it from wiggling around is handy too.
The paper has a fair bit more about this if I’ve piqued your interest. It’s an under-studied topic but I can direct you to more about it if you want was well. Just lmk!
Paper? Indeedy-doody.
And that’s our week!
Here’s hoping you’re having or had a good holiday season and you’ll be hearing from me again next week. Oh, lastly, do share PT Crab with colleagues and whatnot. We don’t advertise, all our growth is word of mouth. So thanks for your mouth! I guess. Bye!
Comments
Want to leave a comment and discuss this with your fellow PTs? Join PT Crab and get summarized PT research in your inbox, every week.