PT Crab 🦀 Issue 168 - Best of Knee

We’re almost to the bottom of the body! Just foot and ankle to go, then one more best of the others and we’ll be back into new content. I hope you’ve enjoyed this dip through the back catalog, I certainly have. It’s brought some interesting stuff to light.
Once we’re done with this loop through Best Of’s, you’ll notice some changes in the Crab as well. I’m moving to a new newsletter platform, so the look and feel will be different. I’ll also be structuring the editions slightly differently in response to some feedback I’ve had from readers. You’ll probably notice some changes and not others, and more tweaks are on the way.
If you enjoy the Crab and want to keep it going, you can always become a paid supporter to help support the PT Crab. That’s $5 per month and gets you three times as many articles as well as a few other things I’ll get into another time. But there are more ways too:
Advertise with the Crab - Have something in PT or health to advertise? More than 1,600 people read this newsletter each week so it’s a great place to share ideas and products. Reply to this email for more.
Hire Me - I write, speak, and more, all in the science and PT space. This includes for clinician-facing content and public-facing as well. If you have a project that could use some effective writing, know someone who is looking for writers, or anything like that, let me know. I specialize in making complex topics simple and understandable. Anyone can email me at Luke@PTCrab.org. Also, if you’re looking for a buddy to help present something at CSM 2025, do hit me up. I’ll happily give it a once-over to see if I can help.
Make a One Time Donation - Don’t want to pay $5 per month? How about just a buck or two every once in a while? If the Crab has been helpful for you and you want to, you can buy me a coffee here.
Tell anyone about the Crab - I’ve started advertising a tiny bit, but all new subscribers come from satisfied ones like you. So tell anyone. Forward this now! Or shout about it at CSM. Or anywhere. If you work in an office with more than one clinician and not everyone is a subscriber, I'm disappointed in you. :(
With all that out of the way, let’s dive in!
Fearful Contractions in ACLR
The Gist - If you’re afraid, according to the Tampa Scale of Kinesiophobia, you’re probably landing differently after your ACLR. At least, if you’re one of these 38 patients who had an ACLR within the last two years. They were compared with 39 healthy controls and had all returned to physical activity and felt confident performing hop tests prior to this study. The researchers used motion capture and EMG to compare the kinematics and muscle activation of the three groups (high fear, low fear, and control) and see just what a difference kinesiophobia made. And there were indeed differences.
At initial contact, trunk, knee, and hip flexion were significantly different between all three groups, with high fear having more trunk flexion than the control group and both high and low fears having more hip and knee flexion. Muscularly, the high fear group had higher biceps femoris activation and higher anterior-posterior co-contraction index scores (i.e. they had more co-contraction around the joint).
In addition to the objective data, they took outcome measures as well, where they saw no differences between the high and low fear groups for the Tegner Activity scale, the International Physical Activity Scale, and the Knee Injury and Osteoarthritis Outcome Score. Though there weren’t differences between the fearful groups, they did score lower than control on all except the Knee Injury and OA scale.
Tell Me More - Equally as interesting as what the researchers saw is what they didn’t see. They had expected to see fear-related differences during the pre-activation phase of the test. Instead, all increased forces were reactive, not proactive. The overall theory is that this increased co-contraction and biceps femoris activation leads to a stiffer joint and less strain on the graft, good things. But they can also lead to increased tibiofemoral compression and knee joint degeneration, bad things.
The lack of difference between the fearful groups in the kinematic variables is notable as well. Both groups tended to increase hip and knee joint flexion, resulting in a lower center of mass. The researchers say that increased knee flexion could lead to “smaller patellar tendon insertion angles, greater hamstrings insertion angles, lower anterior tibial shear force, and lower tibiofemoral peak compression forces, all of which are considered to decrease ACL strain,” so that’s quite a nice adaptation.
The discussion of limitations in this paper and the overall discussion section are very illuminating and easy to read, so if you like ACLR content, do check it out.
Paper? It’s in PTJ, and is open access here.
How to Heal a Hamstring
The Gist - This piece from the JAT (a fantastic journal, btw) presents a straightforward approach to hamstring injury rehab while breaking down some complexity too. They point out that “In the second half of the swing, the hamstring are active, rapidly lengthening, and absorbing energy to decelerate the limb in preparation for foot contact” and that “Hamstring muscle force increases approximately 1.3-fold as running velocity increases from 80% to 100% of maximum and the greatest muscle-tendon unit stretch is incurred by the long head of the biceps femoris.” As folks who know about muscles, you know that it’s dangerous to put out more and more force as a muscle reaches its maximal length. No wonder so many people strain hamstrings.
For diagnosis, they cite research that points out that previous hamstring injury “increases the risk of future… by 2.7 times”. Usually palpation, ROM, and strength testing combine to diagnose the injury. Maximal pain provocation lets one zoom in on the exact location and ROM can provide good indication of tear severity. Lastly, pain rating during isometric contraction and strength of contraction indicate severity as well. In the soccer player paper for King Crab supporters, they use a scale on a box to test strength. The player puts their leg in 90-90 position then pushes down on the scale, forcefully extending their hip and flexing their knee and the maximum value the scale reads indicates current strength. Pretty simple and cool!
Lastly on dx, MRIs haven’t been shown to be too helpful in guiding rehab. In fact, diagnostic ultrasound could be even better, but we don’t have data that shows either as too helpful.
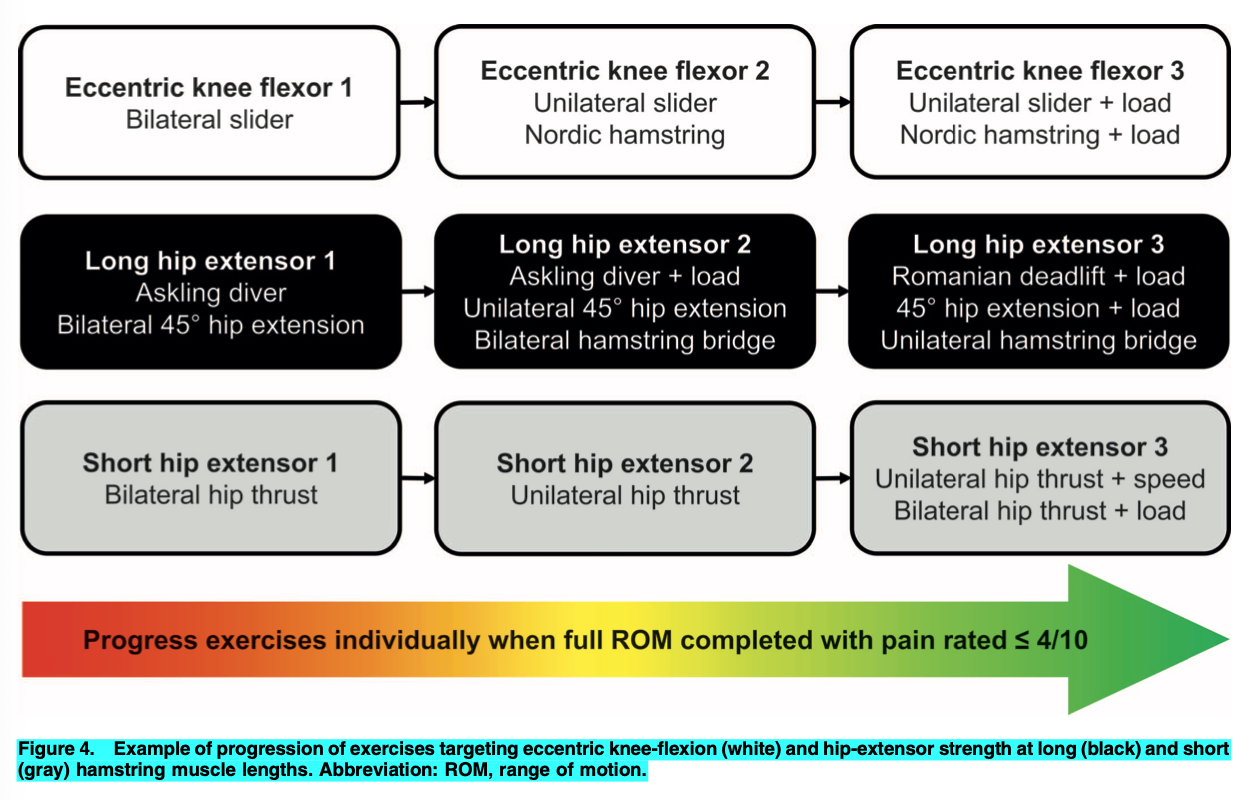
Tell Me More - Now for the rehab. They recommend a 3 stage process for return to running, starting when the person can walk with pain less than 4 on a 0-10 scale. This is gradual progression from slow jogging to moderate running. Then slow progression into faster and faster running with great care taken with exposure to sprinting, only increasing speed 5% at a time as you approach maximal running velocity. For the exercises that help that rehab, they recommend eccentric loading even early in the process. As soon as someone can get through full ROM with pain <4/10, they recommend a combination of eccentric knee flexion, long hip extension, and short hip extension exercises. I included a figure to better define what they’re talking about.
They also have a series of videos showing the specific exercises recommended. Here are links to those:
- Submaximal slider exercises: http://doi.org/10.4085/1062-6050-0707.20.S1
- Hip extensor exercises: http://doi.org/10.4085/1062-6050-0707.20.S2
- Hip thrusts: http://doi.org/10.4085/1062-6050-0707.20.S3
They also recommend progressive agility and trunk exercises that can help control lumbopelvic position and reduce hamstring length in running. Alongside all that, there recommend hamstring flexibility exercises “if deficits persist during rehabilitation, as greater deficits in active knee-extension ROM at RTS have been associated with an increased risk of subsequent hamstring injury” and data shows that “Recovery of active knee-extension ROM can be slightly accelerated by implementing passive hamstring stretching 4 times per day, compared with once daily, starting at 48 hours after hamstring injury.”
Lastly, there’s limited evidence that running technique drills and manual therapy are helpful in most people, jsyk.
I’m out of space except to say that they recommend the Askling H-test to test for pain and apprehension and eccentric strength testing to prep for return to sport.
There’s a lot more in the paper, but I think you’ll agree that’s a lot already. If you want more, read it!
Paper? Here it is.
We Don’t Know Much about Osgood-Schlatter
The Gist - Osgood-Schlatter is a pretty simple condition with a prevalence reported at about 10%, but that’s about all we know about it. The exact cause is unknown and (more concerningly) so is the best treatment. In fact, there are no CPGs on its treatment and published research largely disagrees on what to do. This systematic review wanted to set things straight, but it really couldn’t. There was so much heterogeneity and so few studies (13 in the last 70 years!) that they couldn’t come up with recommendations. They can tell you that most studies focus on activity modification, quadricep and hamstring stretching, ice, isometric quads strengthening, and NSAIDs. We don’t know what to do about it. One bright spot though, we may know how to help prevent it. Single-sport athletes are twice as likely to get it as their multi-sport fellows, so early activity modification can help.
Tell Me More - I mean, there’s not a lot to tell. I’ll leave you with the disappointed words of our authors:
When considering all of the studies and their results, a “consensus” treatment recommendation may be the modification of physical activity. Taping or patellar strapping is frequently recommended, which is similar in motivation to the approach of isometric strengthening of the quadriceps in knee extension and stretching the hamstrings. However, there is a lack of RCTs that provide high-level evidence in favor of stretching or strengthening exercises for the lower extremity in children or adolescents with OSD. Existing evidence on exercise therapies is contradictory and controversial.
So yea, that’s where we are.
Paper? If you want to crawl into a hole of sadness, sure, read the paper. But srsly, it does have some good background on OSD, not much else.
The Internet is Wrong About Your Knees
The Gist - We’re all pretty sure the internet can be a great place and that it can be terrible. If you’ve got PFP pain, it’s closer to the terrible side of that scale. PFP pain affects one in four young adults, but 41% of them don’t see a physician for it. Many of them see Dr. Google and his treatment methods are a bit outdated. Researchers evaluated the first two pages of Google and Bing (don’t laugh! Bing gets 500 million visitors per month, jsyk) for the terms knee cap pain and patellofemoral pain and came up with 40 unique URLs to assess. Here’s the roundup:
- 43% didn’t provide sources
- 38% didn’t provide authorship
- 50% didn’t provide funding
- 45% were created to advertise products and services.
- 20% were wrong about what PTP pain was
- 22% recommended knee surgery.
It’s an ugly playing field out there. But good to know about if you’re hitting resistance to your treatments. 22% of people might think they need surgery for their PFP pain. Yikes.
Tell Me More - I know that things like authorship and sources seem less important than accuracy (and they are, a little) but they’re essential to helping make sure good information rises to the top. Only 15% of websites gave information about appropriate interventions according to current CPGs. 15%! The information out there was so bad that researchers put sites without information into the good column, since at least they weren’t harmful. That’s what we’re up against. But it’s not unbeatable.
You can do something about it as a PT in a few ways, but one is as simple as finding a PT YouTuber you like and liking / subscribing to their videos. Things like this help them rise up in search, getting more accurate information in front of people. Additionally, the Netherlands recently found that a nationwide, evidence-based health website dropped healthcare usage by 12%. Wow! Lobbying for or working on something like that could be huge. Lastly, I know many of you may not like the APTA, especially right now, but they do a lot of this information sharing work and your membership helps pay for it, so consider that when renewal comes around.
Here’s that paper. Right here.
And that’s our week! That was a quick run through some of my favorite knee topics. And hard to figure out which to pick really, since the knee is basically the hip, let’s be honest. But I think these were all knee-centric enough! If you like or don’t like what I wrote today, shoot me an email just by hitting reply.
’Til next time!





Comments
Want to leave a comment and discuss this with your fellow PTs? Join PT Crab and get summarized PT research in your inbox, every week.