🦀 PT Crab Issue 61 - Take BP. Do it. Do it now.

Like seriously, take your patients’ BPs. If you’re not down with this now, you will be after reading today’s second article. Also, Paul Geisler knows what really causes IT Band pain syndrome and soon you will too.
If you’re interested in all PT Crab has to offer and in keeping it alive, please consider becoming a supporter. More details on how to do that here.
Also, today’s the day where night and day are of equal lengths. Welcome to autumn, starting with the equinox. It’s one of two days each year where day and night are a solid 12 hr week. Good for them for learning to share, for a day at least.
Also also, today’s PT Crab is brought to you by Fulton insoles. More on that later.
With that, let’s dive in.
What really causes IT Band Pain? Paul Geisler knows.
The Gist - This fantastic summary by an ATC, Paul Geisler, breaks down the complete history of ITBPS, including the current view of what causes the pain and how to fix it. The history section is incredibly interesting, starting with a description of the IT Band’s first discovery in 1843 and taking us through the entire pathohistorical pathway to understanding ITBPS. But I’m just gonna start with today’s deets, since that’s probably why you’re here.
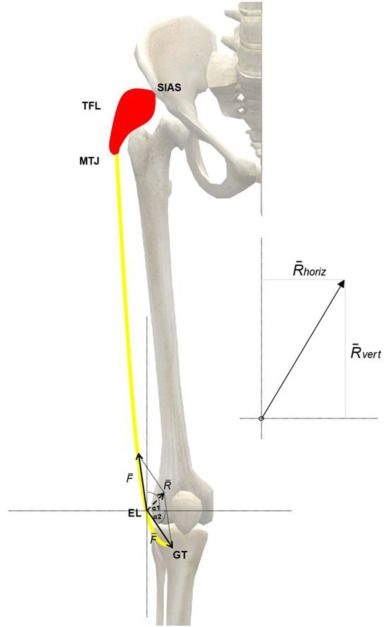
Our current, evidence informed model of ITBPS says that the Ober test does not demonstrate a tight IT band, since the IT doesn’t limit adduction (glute med and min do) and that the IT band cannot be stretched. Even stretching TFL doesn’t help because of the IT’s multiple attachments to lower fascial and bone layers. Nor does the IT band roll over the femoral condyles, for the same reason. Rather, the cause of IT Band Pain Syndrome is related to impaired hip musculature that allows femoral drift into the frontal plane in running, leading to femoral adduction and IR that causes sub-IT fat pad impingement. And since causes took that much room, let’s go to the next session for assessment and treatment.
Tell Me More - Assessment is recommended to be a thorough history that includes recent changes in training volume or any hill running (esp. downhill) and both history and (possibly) palpation that demonstrate sharp, focal lateral knee pain. You can also have the person jog for about 20 minutes on a treadmill and watch for femoral adduction at the end, during the stance phase, demonstrating lack of hip control.
Treatment? The author goes through three levels of management, so I won’t dive into all, but here’s the gist:
- 1 - Low-load, open chain phase focusing on motion control in hip exercises
- 2 - Moderate-load, closed chain phase focused on keeping pain low, increasing endurance, and training hip control
- 3 - High impact, tolerance, and ready phase focussed on sagittal plane control, landing drills, flat ground running, and more
I highly recommend reading the whole paper. So, do that.
Paper? Yupp. Read it. Open access, so highlighted version is here.
Gel Insoles Suck. But there’s an alternative.

The Gist - Do you patients need arch or foot support in their worn out white New Balances? Do you have someone who “wears the same shoe every day, no matter what” and won’t take your advice to change it? We’ve all had that guy as a patient and we know how tough it is to talk them into support. But we also know how important the correct support down there is to everything that they do. Well it’s time to introduce Fulton, a new insole company who want to support you and your patients from the ground up. This is a modern brand of arch support, changing how things are done.

Tell Me More - Fulton uses sustainable materials to produce supportive and comfortable insoles that improve alignment and posture. The cork base absorbs shock and molds to your foot, providing a custom fit, the deep hell cup provides maximal stability, natural latex foam improves comfort, and every piece of the insole is natural and biodegradable. They have free shipping and returns, so every order is risk free.
Learn more and order at WalkFulton.com for a better way to walk.
Link? I mean, it’s right up there, but sure, I’ll put it here too.

Please Check Your Patient’s BPs. Here’s Why and How.
The Gist -This exhortative article comes from PTJ and begs you to take a BP screening if you’re an outpatient therapist. The authors go through a ton of detail and arguments about why this is important and how to do it accurately and cost-effectively, so here are some notes in brief.
- BP measurement should be in a routine exam of all patients
- Only 10 - 15% of PTs measure BP, even in cases of direct access, where they may be the only healthcare provider the patient is seeing
- BP screening is an effective strategy for early detection of HTN
- HTN screening is an ethical duty of care due to HTN’s morbidity, disability, and mortality
- HTN screening is fast and easy to do in outpatient clinics as part of a routine exam
I could go on (and they do and you should read it) but just start screening your patients, okay?
Tell Me More - I already made the major point, so here’s what you need to do it. 1 stethoscope per therapist, 1 standard BP cuff per 2 therapists, 1 small and 1 large cuff per clinic, and 1 thigh cuff just in case. Keep your equipment calibrated by checking it every 6 months (22% of PT’s gauges are inaccurate 😲) and follow a standard protocol when taking BP: seating, rested position for 5 minutes, feet flat on the floor and uncrossed with back supported. None of that legs off the plinth nonsense, it can throw you off by 8mmHg. Tell that patient to shut their mouth too, talking can mess things up by 15mmHg. Wow.
The paper also goes into some great discussion of why PTs should be measuring BP response to exercise. Mainly, PT is the only place that most patients will even have the opportunity to exercise near a healthcare provider (and the only place where many will exercise at all) so it’s a perfect time for screening that’s easier than a real stress test but can still show pathologies. The Crab has previously covered hypotension and why that’s a big problem, but obviously, hypertension is bad too. So take BP people! The paper has more details on when, how, and why. Give it a quick read, it’s worth your time.
Here’s that paper - It’s open access too. Yay!
And that’s all she wrote. Thanks again for subscribing and sharing PT Crab. It’s been slowly growing over the last few months and you’re our only advertising, so thanks for your word of mouth. If you want your boss to pay for a premium subscription, we have a plan for full clinics as well, just have them email me at Luke@PTCrab.org
Cheers!



Comments
Want to leave a comment and discuss this with your fellow PTs? Join PT Crab and get summarized PT research in your inbox, every week.