🦀 PT Crab Issue 110 - ACLR and All Involved

This week’s PT Crab is brought to you by Unspun. Details below.
This week we’re popping into a well-trodden topic in the PT world, but not the PT Crab world. It’s ACL rehab. But I’m still taking the PT Crab spin on it since I assume you know how to treat this condition pretty well already. Outside of the fact that open-chain exercises for ACLR rehab seem basically fine, not much has changed in the PT approach over the last few years. What we’re looking into instead are the psychological and emotional sides of ACL rehab. Most people who tear their ACLs don’t return to their prior level of sporting prowess (see below). There are many reasons for this, but the psych element can’t be overlooked. So read on for more detail on that.
King Crab supporters (who help out for just $5/month) also get access to two more articles this week, so they dig a lot deeper into that topic. See the details of what you get as a supporter and sign up here.
Also this week, don’t miss fall foliage y’all. Seriously. Go look at some leaves. Take a hike. Literally.
With that, let’s dive in!
What are patients really saying? Listen between the lines.
The Gist - Researchers in the Journal of Athletic training wanted to learn more about how to support patients in the long process of ACL repair using qualitative interviews combined with patient reported outcomes to find out what patients were thinking as they recovered. In their words, “Capturing these…components is important because negative psychological responses may act as barriers to successful rehabilitative outcomes after ACL.” Here’s what they found:
Based on outcome scales, subjects were split into high and low perceived disability groups. Those in the high group had more internal and external barriers, like fear of reinjury and feelings of incapacity (internal) and limitations in coverage of treatment or treatment availability (external). Low disability groups tended to have more family and/or team support and an internal locus of control that high disability groups lacked. Those in the high disability group tended to have more emotional concerns, like depression and anxiety, though the study didn’t differentiate between depression acquired due to the injury and pre-existing depression.
Tell Me More - There’s a lot more in this open access paper so I highly recommend a full read. They use patient quotes to emphasize points and they’re quite powerful.
I think more mentally than physically, like I’m still cautious. The fear of retearing my ACL or doing something to screw up my surgery—I haven’t even gotten on a mountain bike since before my surgery because, is that one ride really worth being on crutches?
All patients, regardless of disability status, expressed negative emotional factors about some point of the process. Most patients expressed mental blocks to activity participation and fear of reinjury, but those in the low disability group were more effective at overcoming these feelings, though their methods of doing so remain opaque.
The biggest differences between the high and low disability groups were the facilitators to rehab. These were an internal locus of control, a stable support network, clear expectations of the recovery process, and fewer limitations during immediate postop rehab. Of all these, the largest difference that we can make as PTs is in clarifying the recovery process from day one. There’s a significant amount of misinformation about ACL rehab out there (like people returning to the field in 6-9 months, it happens but it’s not the norm) and we can go a long way toward closing the info gaps with our patients.
Much more in the paper - Open access here.
unspun makes jeans for you. Just for you.
Seriously. They 3d scan your body for them. And you can get $40 off these premium jeans by being a product tester.

Lots of companies make jeans. Lots of companies makes jeans for you. Only unspun makes jeans just for you. They guide you through a 3D scan of your body, then make jeans designed to fit just you and fit you perfectly. They're $200 jeans, a premium product, and they're unique to your body. No two pairs are alike.
If you're someone like me, with big hips and a trim waist, you know the struggle to get jeans that fit without having to pull them up every 47 seconds. unspun fixes that problem.
unspun is an ultra-sustainable denim brand, building custom-fit jeans for each customer from a 3D iPhone scan. Just choose a style & fabric, and unspun takes care of the fit by designing to the unique shape of your actual waist, hips, and legs. They guarantee their $200 jeans will be the best-fitting pants you’ve ever worn (or they’ll take them back and buy you a coffee), and are looking for a few early product testers to give them feedback on the experience in exchange for a $40 gift card towards your first pair.
Get that deal and support PT Crab by clicking here.

From the Archives: You Can Trust Your Patient’s Subjective
The Gist - A couple of PTs from Tufts University wanted to see if patient histories were well associated with diagnoses when it came to hip pain. Good news, they were! These researchers went through dozens of articles to extract information from 9 studies that included patient history and eventual diagnosis. Through some complicated data crunching, they were able to turn self-reported info into likelihood ratios for Hip OA, making it that much easier to diagnose the condition. Don’t remember what likelihood ratios are? Check the Tell Me More section below.
Here are those ratios. Remember, they’re all for the diagnosis of Hip OA
Patients who reported a family history of hip OA had a positive LR of 2.13, family history of knee OA is an LR of 2.06, limited ROM in one or both hips is 2.87, constant low back pain or buttock pain gave a 6.50, and groin pain on the same side gave a 3.63. Considering that the classic, FABER test has a positive LR of just 1.9, these are great numbers.
Tell Me More - So what is a likelihood ratio again? Yeah. They don’t come up too much after most people leave school. Basically, likelihood ratios increase the probability of someone having a condition. There’s a complex way of actually figuring out exact numbers by using a nomogram to compare pre and post-test probabilities but that’s just silly to use in your clinic. Instead, I offer you a much easier chart.
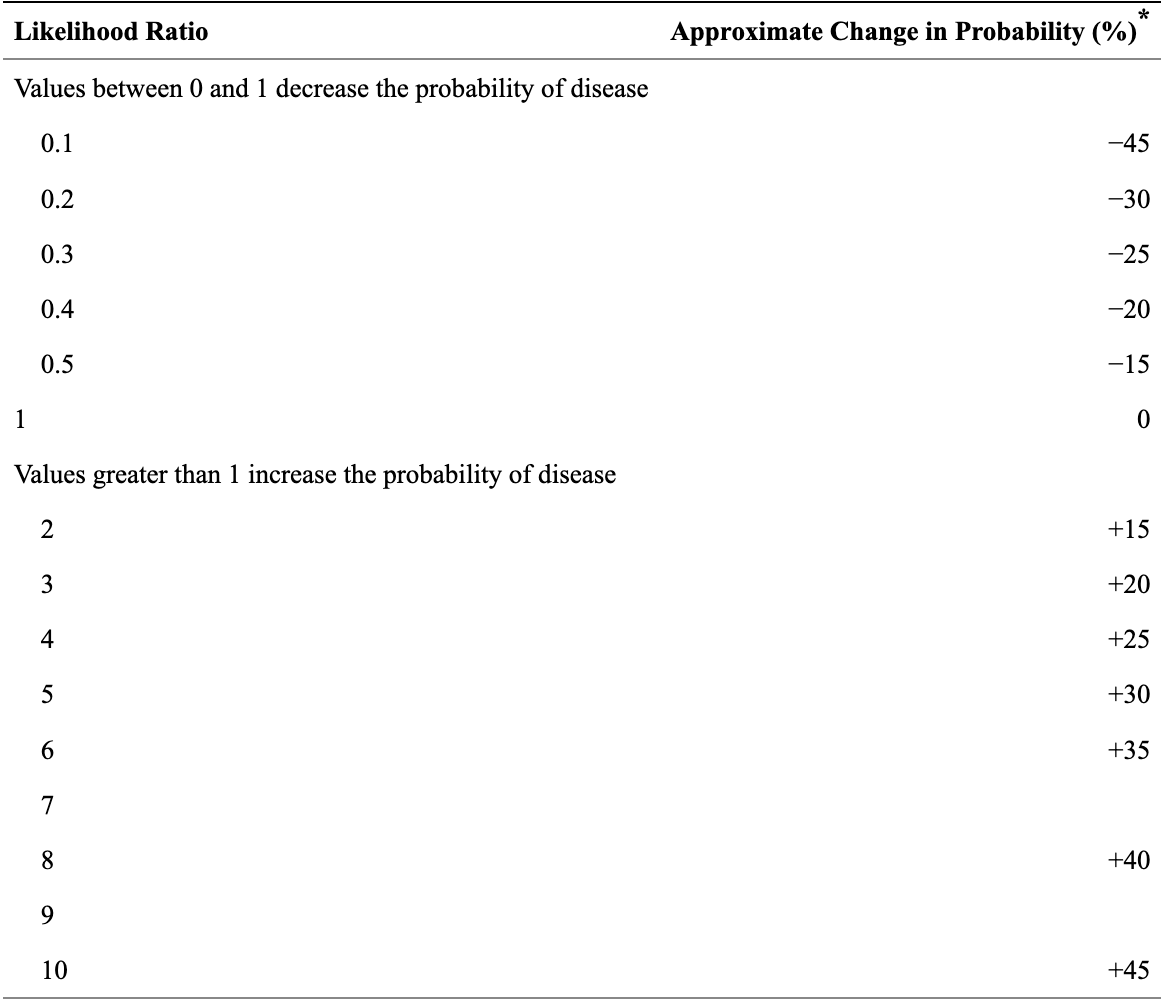
Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1495095/table/tbl1/
So if someone has constant low back pain or buttock pain, their probability of having Hip OA increases by about 35%. That’s huge! This still relies on you having a pre-test probability in your mind before the subjective, but I’ll bet you already did anyway, didn’t you?
For more from the actual paper, there was no history obviously associated with FAI or labral pathology and only one associated with intra-articular pathology. This was crepitus, giving a positive LR of 3.56 (increasing probability by about 22%).
Overall, this paper makes a strong argument for taking a great history, so be sure your skills are on point. They say that “Multiple studies have reported that patient history alone has upward of 75% accuracy in determining patient diagnosis before performing a physical examination.” Wowza. Especially today, as telehealth becomes more common, patient histories are huge.
Can I see the paper? Sure thing boss. It’s right here.
And that’s our week! Hope you enjoyed. Please share with friends, colleagues, frenemies, enemies, etcs. Just forward this email to them. And remember that PT Crab is Con-ed in a few states (6 I think, double-check here) so your clinic may even pay for your subscription out of their con-ed budget. Yay!
Have a great week,
Luke





Comments
Want to leave a comment and discuss this with your fellow PTs? Join PT Crab and get summarized PT research in your inbox, every week.