Issue 19 Blue Crab Edition - An RCT Hip Mobilization with Movement in Hip OA and the Real Structure of Vastus Medialis
This week’s Blue Crab edition of PT Crab focuses on the hip and knee as we take a tour of the vastus medialis muscle architecture to find that it’s much more complex than we think and find out how mobilization with movement can help patients with hip OA. It’s a deep cadaver study and an RCT this week, so we’ve got variety in spades.
King Crab subscribers got two more articles this week (as usual). There was a second MWM study about its effects on shoulder motion in people with impingement syndrome and a piece about recognizing and correcting gait problems and ankle coordination in people with chronic ankle instability. Get the full edition at PTCrab.org/Subscribe.
With that, let’s dive in!
MWM Decreases Pain and Increases Mobility in People with Hip OA
The Gist - This RCT claims to be the first to look into the immediate effects of mobilization with movement on hip OA and they’re looking pretty positive so far. They randomized 40 patients to MWM or sham treatment, then performed hip flexion MWM and IR MWM to the MWM group. The sham people got a sham version. Immediately afterward, they reassessed pain, range of motion, and a few functional tests.
MWM decreased pain by two points on a 0-10 scale, increased hip flexion range by 12.2°, increased IR by 4.4°, decreased TUG time by 2.7 seconds, and decreased the 40m self-paced walk time by 11.2 seconds compared to sham. Great results overall.
Tell Me More - The paper itself has more details about the specific techniques used, so grab the link below if that’s what you’re into. Here, we’ll talk limitations and why MWM may have helped these people. First, the why.
MWM’s mechanism is not yet known, but there are a bunch of suggestions offered up by the paper: stretch effect on the joint capsules and tissues to restore normal arthrokinematics, altering a joint’s positional faults, changing the pain inhibitory system, or stimulating joint mechanoreceptors. There are others as well. Like much of manual therapy, we don’t really know why yet, we just know that it works.
Speaking of if it works, limitations. This study was pretty small and doesn’t have much corroboration. As I said above, it’s the first of its kind. On the plus side, it was double-blinded in the randomization phase and in data analysis, so that’s a big plus. They only evaluated immediate effects, and only one session of treatment was applied. Lastly, in order to seek specificity, they didn’t combine this with any other treatments, potentially limiting generalizability. Hey, you can’t have it all.
Paper? - It’s here and open access. Enjoy!
What is Vastus Medialis Really Like? Weird.
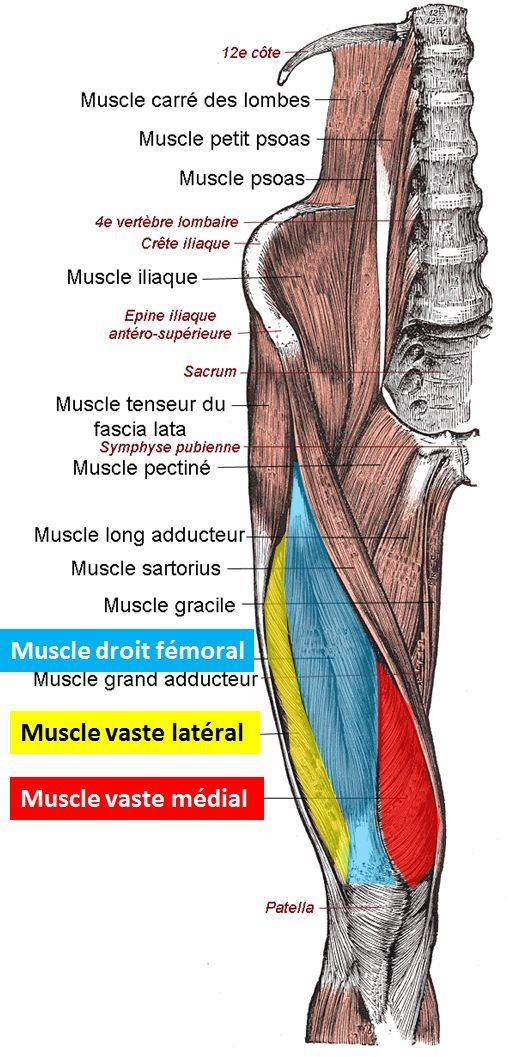
The Gist - Cadaver studies don’t often feature in PT Crab, since there’s rarely anything clinically applicable, but this interesting study may have some clinical nuggets. They assessed 18 cadaveric lower limbs to study the anatomical interaction between VM and VI and came up with some cool stuff. VM is a clamp muscle. Strange, huh? The figures in the paper really make it clear, so I highly recommend checking those out. I’ll try to explain below.
VM originates from the medial surface of the femur and has most of its fibers directed transversely across the bone, then wrapping around the VI aponeurosis “like a clip holding a sheet of paper.” It uses this clipping action to pull the VI medially while it contracts, changing the direction of force on the patella. Cool! VM also has an insertion on the patella, so it doesn’t only pull VI, but that’s a function of it.
Tell Me More - Let’s talk about why this matters. The researchers point out that this is new information about VM and that it digs deeper into how the muscle controls patellar motion. In their words, it “functions as a dynamic medial stabilizer of the patella”, not via direct pull on the patella via the distal, VMO portion, but mostly through its control of VI’s direction of pull. They also note that this study, combined with previous ones, shows that direct force supplied by VM for knee extension is limited. Specifically:
The EMG observations in the literature, together with findings of the present anatomical study, suggest that the VM acts as an indirect extensor at the knee. It can be hypothesized that by pulling the longitudinal components of VI and rectus femoris medially and dorsally, the VM tight- ens and shortens these quadriceps muscles, much like a belt around the waist. Obviously, this shortening of the length of the quadriceps (indirect extensor mechanism) is most important during the terminal phase of extension.
This is some interesting new ground in our understanding of knee extension. Check out the full paper for the figures and more details about their new findings.
Here’s That Paper - And it’s open access! Yay!
That’s all we have for this week, but I think we can safely say that it was a lot and quite valuable. Please send me any opinions, ideas, or otherwise that you have about PT Crab, by emailing Luke@PTCrab.org. I’m always happy to hear from you. As always, share this far and wide. We want to democratize PT research and can’t do it without you.
Cheers,
Luke
Feature image: Didier-CTP, CC BY-SA 4.0 https://creativecommons.org/licenses/by-sa/4.0, via Wikimedia Commons





Comments
Want to leave a comment and discuss this with your fellow PTs? Join PT Crab and get summarized PT research in your inbox, every week.