🦀 Issue 56 - Who was Colonel Vogel?
Howdy ya’ll! Welcome to August, a time of angst amongst many as we all prepare to go back to school or send our kids that way. Want to alleviate some of that? I’ve got another podcast for you! (Hey, I listen to a lot, don’t judge) This one’s called Detours and it’s from the team behind The Antiques Road Show and is produced by PRX and WGBH so it’s a high quality property. They look into the stories behind the scenes and behind the items from TARS and it’s a fantastic show. They’ve only done one season so far, but it was great. Check it out when you get a chance.
With that, let’s dive in!
Get Your Brain Right
The Gist - There’s more to return to sport the physical readiness. This is something we all know, but it doesn’t really come up in standard tests. To dig deeper into it, a team of Japanese researchers in the journal Physical Therapy in Sport grabbed 50 athletes between ages 16 and 45 and had them take the ACL-RSi, a psychological readiness questionnaire designed just for this purpose. They got a pre-op score and a 6 month post-op score and were able to categorize their participants based on them. After analysis, they saw that the 34% of their participants that had low pre-op scores also had lower 6 month post-op scores, while those who had high pre-op scores tended to do better postoperatively and return to sport sooner.
Tell Me More - I know that’s just data, here’s what it means. Patients who were less psychologically “fit” pre-operatively stayed that way post-op and had a harder time feeling ready to return to sport even after they should have been prepared for it. Meanwhile, those with more psychological fitness got psychologically ready more quickly. The researchers say that this is interesting data since it points to a practitioner’s duty to assess psychological readiness early in the rehab process. This could show them a patient’s likely psychological path through rehab and detect problems that may predict poor outcomes.
Paper? Sure! Though it’s been translated from Japanese and not beautifully, so it’s a bit of a tough read. It’s here.
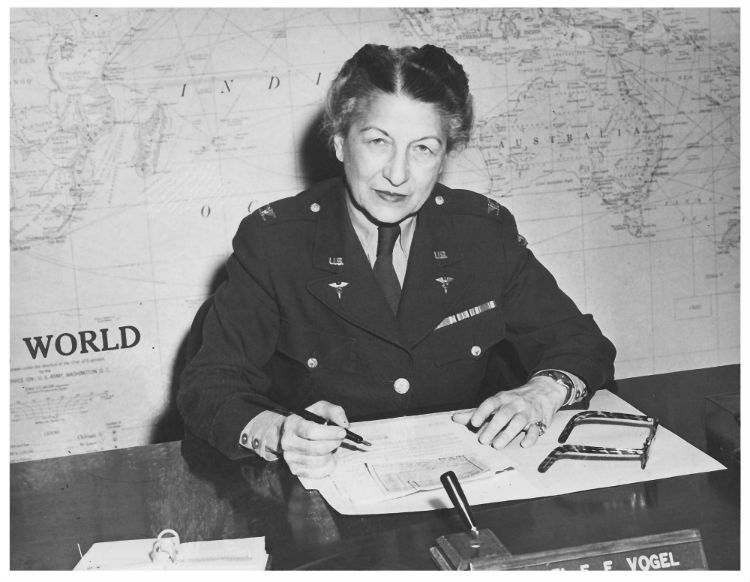
Who Was Colonel Emma Vogel?
The Gist - PTJ recently ran an open access piece about Colonel Emma Vogel, one of the first physical therapists in the US Army and the very first one at Army General Hospital near Pittsburgh, PA in 1919 (though, technically they were called Physiotherapy Aides until she convinced Congress to change that in 1944). She served at Walter Reed amongst many other places and was one of the leading educators of PTs before the Second World War. In her career she treated thousands of patients, educated hundreds of PTs, gave lectures, helped stop discrimination against male PTs in the military, received awards, and more. The Colonel died 40 years ago last week at her home in St. Petersburg, FL and was buried with honors at Arlington National Cemetery.
Why am I telling you this? Because she was an amazing woman and it’s important to know the history of your profession. Check out the full piece to see all she did. It’s a brief two pages.
Paper? Yupp. Open access here.
Will You Resprain that Sprain? Yes, but less if you’re female.
The Gist - You ever read a research paper and just go “wow, that must have taken a ton of work!” No? Just me? Well, regardless, this one definitely did. Researchers publishing in the Journal of Athletic Training (my favorite journal! Seriously.) wanted “to evaluate the evidence regarding the association between lateral ankle sprain history and subsequent LAS risk, as well as sex differences in the observed associations.” And boy did they. From reviewing 19 studies that had 6,567 patients, they were able to see that prior lateral ankle sprain provides a 3.56 relative risk for future sprain if you’re male and 2.4 if you’re female. You also have a higher risk of respraining if you’re not an athlete. Clinically, this matters, I promise. Read on for more.
Tell Me More - The authors themselves point out that
These results highlight the importance of (1) preventing the index LAS (ie, primary injury prevention) and (2) emphasizing the need for rehabilitative strategies (ie, secondary prevention programs) to prevent negative long-term health outcomes after an LAS…. Rehabilitative programs intended to prevent recurrent LAS are hampered by an erroneous public perception that LASs are inconsequential injuries that do not need rehabilitation. Indeed, fewer than 7% of patients with LASs complete any physical therapy within 30 days of their injury. Also, patients who did not seek medical care for their LASs described a greater number of recurrent LASs and worse patient-reported outcomes than those who participated in formal medical care.
Sharing results like these with the general population can help convince more people to take ankle sprains seriously. I had dozens (literally dozens) when I was a kid and only sought PT once. Ouch. Literally ouch. Since the research showed that those who seek treatment as less likely to reinjure than those who don’t, share this news far and wide.
Paper? Sure sure sure. Open access here.
Exercise Works for PFP and More Exercise Works More
The Gist - Guidelines for PFP treatment have come about fairly recently (back in 2016 at the International Patellofemoral Pain Research Retreat (which apparently exists, who knew?)) and these researchers wanted to put the exercise guidelines to the test. To do so, they got 27 people with PFP, tested them, gave them exercises for 6 weeks, and retested them. You know, the standard stuff. (For those of you playing study bingo at home, this is an observational study). 16 of their participants actually finished the whole thing and the data showed that the exercise plans were effective at improving function, reducing kinesiophobia, and decreasing quadriceps AMI (that’s anthrogenic muscle inhibition, jsyk). They weren’t effective at decreasing pain, but that’s because pain started at 0.9 and the MCID for it is 2. Gonna be tough to decrease that meaningfully… This was a small study, I know, but it’s one of the first to directly take these recommendations and rest them, so it’s important. What exercises did they do? Coming right up.
Tell Me More - They gave each participant 4 exercises and 2 stretches and advised them on how to advance the exercises throughout the process. These were 1) A squat, 2) A bridge, 3) side band and rotational walks with a theraband, and 4) open chain quad strengthening. The stretches were for hamstrings and gastroc.
So where does this leave us? A bit in the Neverwhere. The exercises that were given didn’t increase quad strength, implying that they were too easy, but the participants did get a bit better across the board. The researchers were concerned that really hard exercise would trigger PFP pain, so they recommend that others try these with BFR in future to get the strengthening without the pain. Overall, this is a weak study, but it’s testing something pretty new and we’re slowly building up data about it. Only time will tell if this is the best treatment in future. In the meantime, check out those 2016 recommendations and read this paper if you want to.
I want to. And I won’t stop you. But the paywall might…
That’s our week! Do check out Detours, it’s a great show. Thanks again for being a PT Crab supporter, it means a lot. Always feel free to email me with questions, concerns, ideas, etc. I’m always happy to hear from you. Luke@PTCrab.org Also, you know, like keep sharing PT Crab. It’s how we grow.
Thanks, bye.





Comments
Want to leave a comment and discuss this with your fellow PTs? Join PT Crab and get summarized PT research in your inbox, every week.